
Horizontal GBR in the posterior mandible, using the L-prf bone block protocol
Dr. Stefan Matthijs, Periodontist
Belgium
Patient: 57-year-old female, no systemic diseases, no oral pathologies
Clinical situation: Tooth 46 (FDI) was removed 8 months earlier. Missing lower molars 46 and 47. Reduced masticatory function. Horizontal bone deficiency and reduced soft tissue volume.
Surgical planning: Horizontal bone regeneration, prior to implant placement.
A mixture of small and large size Nobel Biocare creos™ xenogain granules and L-prf was used to create a soft bone block. The bone substitute was covered by a Nobel Biocare creos™ xenoprotect resorbable membrane and L-prf membranes. No pins were used to stabilize the membrane. The need for soft tissue augmentation was evaluated at a later timepoint.
Prosthetic planning:
Individual screw retained crowns on implants
Chronology of the treatments:
27th of April 2017: Guided bone regeneration
10th of November 2017: Implant placement
25th of January 2018: Evaluation of the integration – start of the prosthetic treatment
9th of August 2018: First clinical and radiological evaluation of the final reconstruction
24th of October 2022: Clinical and radiological evaluation during the yearly supportive implant care visit.
Total treatment time:
10 months - 5-year follow-up
Tooth position:
Right lower molars, 46 and 47


Tooth 46 was extracted 8 months earlier.
Missing occlusal contact with tooth 16 and 15.

There was an obvious deficiency of the hard and soft tissues.
Limited width of the keratinized mucosa was visible, especially at site 46.

The cone beam CT image of site 46 and 47 showed the reduced width of the alveolar bone. This would make an optimal prosthetically driven implant placement impossible.
The vertical crestal dimensions were favorable.

Cone beam CT images of site 46 and 47. The sagittal view showed sufficient alveolar bone height (left)
The axial view demonstrated a lack of alveolar bone at the buccal aspect of the residual ridge. This defect was more pronounced at site 46 (right).

A full thickness flap was raised without releasing incisions and revealed the amount of the buccal bone resorption (left).
The receptor bed was modified by perforating the cortical bone (right).

After venipuncture and centrifugation of the tubes, the L-prf membranes were prepared.

Several L-prf membranes were cut to smaller pieces (left).
These were mingled with liquid fibrinogen and a mix of small- and large-size creos™ xenogain granules. This produced the typical “sticky bone,” which is easy to handle during the augmentation procedure (center).
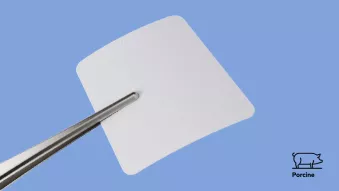
The creos™ xenoprotect resorbable collagen membrane, prior to adaptation (right).

After positioning the membrane at the buccal aspect of the jaw, the soft bone blocks were packed between the membrane and alveolar bone (left).
The collagen membrane was carefully adapted over the graft (right).

Two L-prf membranes were used to cover the collagen membrane in order to support wound healing and stimulate angiogenesis.

Tension-free closure of the flap was obtained with double-loop and continuous sutures (left).
The PTFE creos™ syntostitch (Cytoplast™) sutures (4-0) were removed after 11 days (right).

Six months after the initial regenerative surgery, a new cone beam CT analysis of site 46 and 47 was done. These images demonstrated the gain in bone width at both sites.

Simulation of an implant (10 mm x 4.3mm, RP) at site 46 and 47, before and 6 months after the bone regeneration procedure.

The periapical image showed a limited vertical displacement of the graft material. The axial CBCT image demonstrates the substantial gain in bone width.

Three-dimensional reproduction of the regenerated buccal bone volume.

After crestal incision, a full thickness flap was raised, revealing solid buccal bone with some loose superficial bone particles.
During careful implant bed preparation, the integrity of the regenerated bone wall was preserved.

The implant bed was fully prepared and two NobelParallel™ Conical Connection 4.3 mm (Regular Platform) implants were installed.
Stability values: implant 46 = torque 35 Ncm – ISQ 76 / implant 47 = torque 30 Ncm – ISQ 70

Two healing abutments (5 x 3 mm) were installed, and the flap was sutured without adaptation of the margins.
The amount of keratinized mucosa was considered to be sufficient.

Periapical radiograph taken at the day of implantation and after 3 months of integration. There was only minimal crestal bone remodelling.

The restorative treatment was performed by the referring dentist (Dr. Siska Walraet).
Two screw-retained crowns (layered porcelain on zirconia - Forma®) were made on individualized titanium abutments (Elysee Dental Belgium).
Six months after installation of the crowns, the clinical images showed healthy peri-implant conditions.

The patient’s oral hygiene level was acceptable (left).
The periapical radiograph showed a favourable abutment design, and stable marginal bone levels around the implants (right).

During the yearly supportive implant care visit, the clinical peri-implant parameters are checked and the oral hygiene level is evaluated.
Five years after implant placement, the clinical image shows stable soft tissue adaptation (left).
The periapical radiograph demonstrates stable marginal bone levels (right).
References
- Leucocyte- and platelet-rich fibrin block for bone augmentation procedure: A proof-of-concept study. Cortellini et al., J Clin Periodontol,2018;45:624–634.
- Individual “alveolar phenotype” limits dimensions of lateral bone augmentation. Quirynen et al., J Clin Periodontol,2023,50:500-510. Leukocyte- and Platelet-Rich Fibrin in Oral Regenerative Procedures.
- Quirynen M. & Pinto N.R., 2022, Handbook, Quintessence Publishing, UK.
-
 NobelParallel™ Conical Connection
NobelParallel™ Conical ConnectionA simply straightforward implant system.
Exceptional versatility for universal use. -
 creos™ xenogain
creos™ xenogain3 methods of application to meet all your bone grafting needs.
-
 creos™ xenoprotect
creos™ xenoprotectA membrane with outstanding handling that facilitates bone gain.



Share this clinical case
Sign up for our blog update
Get the latest clinical cases, industry news, product information and more.
© Nobel Biocare Services AG, 2024. All rights reserved. Nobel Biocare, the Nobel Biocare logotype and all other trademarks are, if nothing else is stated or is evident from the context in a certain case, trademarks of Nobel Biocare. Please refer to nobelbiocare.com/trademarks for more information. Product images are not necessarily to scale. Disclaimer: Some products may not be regulatory cleared/released for sale in all markets. Please contact the local Nobel Biocare sales office for current product assortment and availability. For prescription use only. Caution: Federal (United States) law restricts this device to sale by or on the order of a licensed clinician, medical professional or physician. See Instructions For Use for full prescribing information, including indications, contraindications, warnings and precautions. Nobel Biocare does not take any liability for any injury or damage to any person or property arising from the use of this clinical case. This clinical case is not intended to recommend any measures, techniques, procedures or products, or give advice, and is not a substitute for medical training or your own clinical judgement as a healthcare professional. Viewers should never disregard professional medical advice or delay seeking medical treatment because of something they have seen in this clinical case. Full procedure is not shown. Certain sequences have been cut. Dr. Tabanella is a paid consultant for Nobel Biocare. The opinions expressed are those of the doctor. Nobel Biocare is a medical device manufacturer and does not dispense medical advice. Clinicians should use their own professional judgment in treating their patients. Individual patient results may vary.